Initiating Counseling Treatment
Background
As soon as a patient is identified with opioid use disorder, it should be addressed to ensure efficient access to evidence-based treatment and support services. Left untreated, opioid use disorder can result in a decline in mental and physical health, adverse social and economic consequences, and elevated risk of overdose and drug-related mortality.
Select map to display
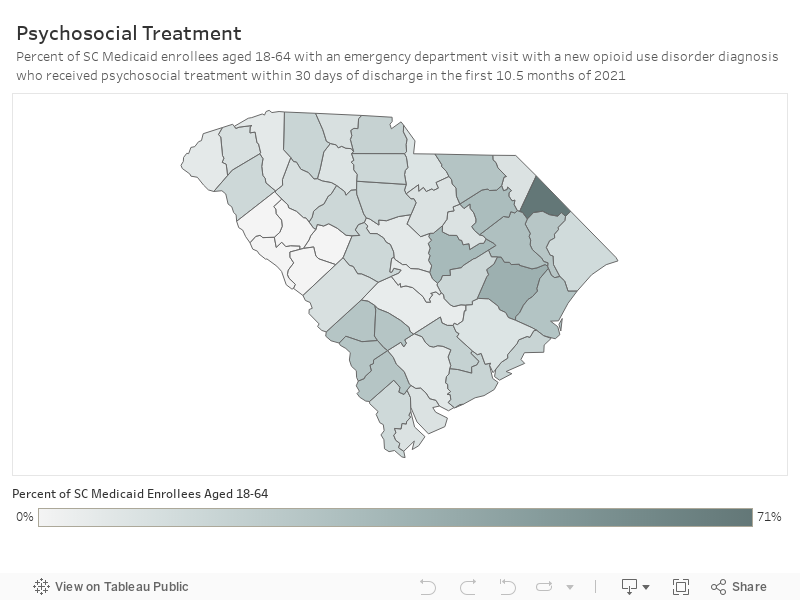
Percent of SC Medicaid enrollees with a new OUD diagnosis:
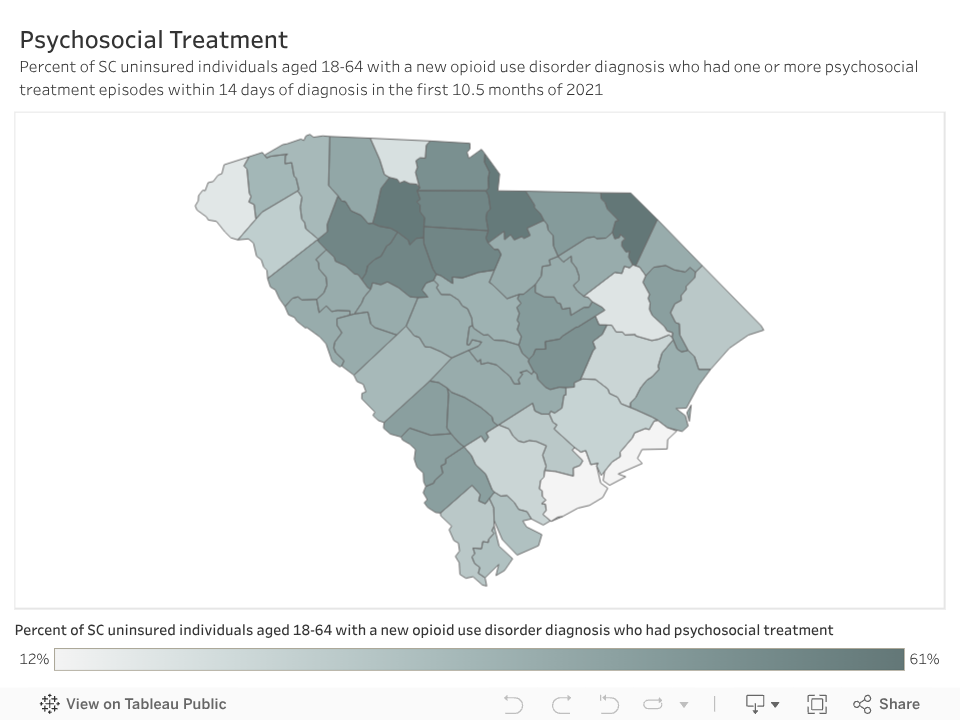
Percent of uninsured SC individuals with a new OUD diagnosis:











Background
As soon as a patient is identified with opioid use disorder, it should be addressed to ensure efficient access to evidence-based treatment and support services. Left untreated, opioid use disorder can result in a decline in mental and physical health, adverse social and economic consequences, and elevated risk of overdose and drug-related mortality.
A wide range of psychosocial interventions have been found effective for treating opioid use disorder, including cognitive behavior therapy, contingency management, and motivational interviewing and relapse prevention. Psychological treatment is most effective when used in combination with medications to treat opioid addictions.[i] Receipt of medications for opioid use disorder treatment should not be contingent on whether an individual is engaged in psychosocial treatment. Treating opioid use disorder with medication is evidence-based; those with opioid use disorder should begin medication immediately with or without concurrent psychosocial treatment.
How this Dashboard Measures Psychosocial Treatment Initiation
Only people with a new opioid use disorder diagnosis (i.e. no opioid use disorder diagnosis or treatment for the preceding 2 months) are included in these measures. These measures are adapted from National Committee for Quality Assurance’s (NCQA) Healthcare Effectiveness Data and Information Set (HEDIS) measures, which are widely used insurance plan performance measures. HEDIS measures are validated, claims-based measures that give a standardized format to compare health system and plan performance across states and years. The NCQA and National Quality Forum (NQF) provide guidelines for creation of these variables that help standardize measures across plans, states, and research teams. Cutoffs and windows for inclusion – such as 14 days, 34 days, and 10.5 months – are based on clinical consensus from NCQA research and HEDIS measure development. We identify treatment two ways. The first is by using opioid use disorder specific treatment codes, such as those that specifically mention counseling for opioid use disorder. The second is by identifying more general codes, such as for psychosocial therapy, used in conjunction with an opioid use disorder diagnosis code during the same visit. The best opportunity to engage a patient in treatment is immediately following initial diagnosis. Early engagement with treatment decreases risk of overdose and death.
Story Behind the Data
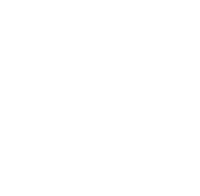
Fewer than one third (27%) of adults with a new opioid use disorder enrolled in Medicaid, and about a third (32%) of uninsured adults, received timely psychosocial treatment.
Among South Carolina adults enrolled in Medicaid or uninsured who are aged 18–64 with a new opioid use disorder diagnosis in 2025:
- Medicaid adult enrollees:
- 27% completed an initial psychosocial treatment session within 14 days
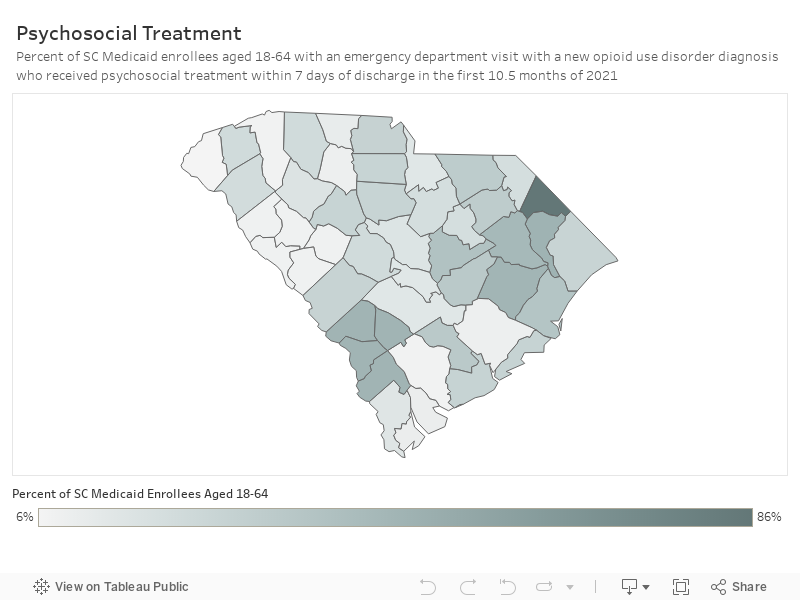
- 18% completed two or more sessions within 34 days
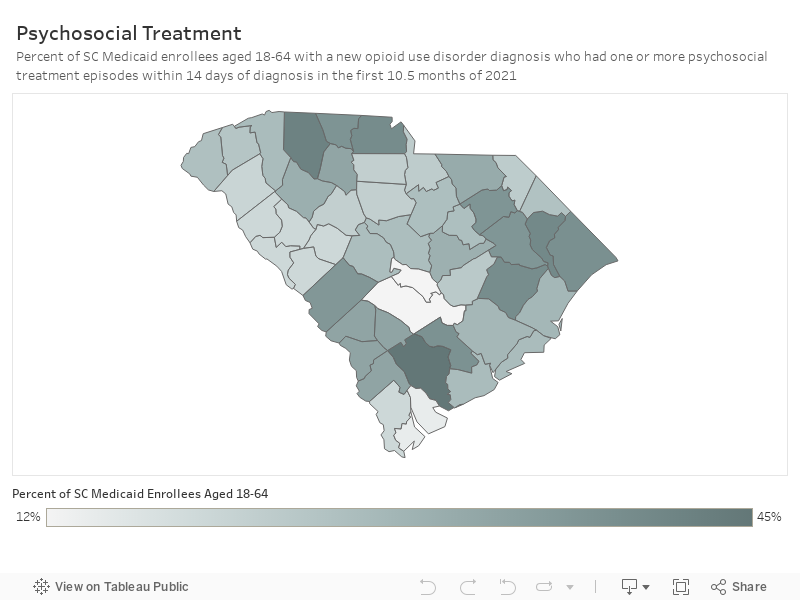
- Uninsured adults (who received care in County Alcohol and Drug Authority or Opioid Treatment Program or the emergency department):
- 32% completed an initial session within 14 days
- 25% completed two or more sessions within 34 days

In summary, of South Carolina Medicaid enrollees aged 18-64 with a new opioid use disorder diagnosis in 2025, about one in four people received psychosocial treatment in a timely manner. Of uninsured adults who received a new opioid use disorder diagnosis at a County Alcohol and Drug Authority or Opioid Treatment Program or an emergency department in 2025, fewer than one in three received psychosocial treatment in a timely manner.
In other words, 73% of Medicaid enrollees and 68% of uninsured with opioid use disorder are not receiving timely psychosocial treatment.
These data also show that opioid use disorder psychosocial treatment initiation rates vary substantially across counties in the state. Rates of initiation in psychosocial treatment within 14 days of diagnosis ranged from a low of 0% to a high of 93% across South Carolina counties. Rates for engagement—completing at least two psychosocial treatment episodes within 34 days of diagnosis—ranged from a low of 0% to a high of 93%. Psychosocial treatment rates fell from 2021 to 2025, but this drop likely reflects barriers to treatment access rather than improved outcomes.
What Works
Despite the strong evidence for the effectiveness of opioid use disorder treatment, there are numerous barriers that prevent individuals from initiating treatment.19 Additionally, many of those with opioid use disorder do not perceive themselves as needing treatment. A multi-pronged approach is needed to increase rates of initiation of evidence-based psychosocial treatment for opioid use disorder.21,22 Evidence-based strategies to improve initiation and engagement in opioid use disorder treatment after diagnosis include:
- Build effective referral systems and warm handoff programs guided by the principle that there is “no wrong door” to initiate treatment. Improving connections to care for opioid use disorder involves viewing health care as a series of chances to engage with patients. Instead of focusing solely on directing patients to the appropriate services, this approach emphasizes recognizing and addressing patient needs in every healthcare, social service, or other service-related interaction. For example, emergency departments, primary care clinics, jails, harm reduction programs, and resource centers can all serve as effective points of contact with treatment services. The South Carolina Department of Alcohol and Other Drug Abuse Services provides helpful information about treatment options and other resources and can be reached by calling the agency at 803-896-5555 or sending a message online.
Additionally, Just Plain Killers and DAODAS provide maps of statewide networks of local providers treating opioid use disorder. - Decrease barriers to treatment by increasing telehealth options and mobile medications for opioid use disorder treatment programs. Barriers such as lack of transportation or childcare can make it challenging to access necessary services for engaging in opioid use disorder treatment. When logistical challenges are addressed, patients are more likely to attend appointments and adhere to treatment plans, leading to better outcomes. Additionally, reducing these barriers fosters a more supportive environment, encouraging patients to seek and remain in treatment consistently. Increasing telehealth options and mobile methadone and buprenorphine programs can reduce common barriers to care and reach people in need across larger distances.
- Implement harm reduction programs to reduce health and safety issues associated with drug use (syringe services and naloxone distribution programs). Programs and practices that aim to reduce the harms associated with the use of drugs include those with a focus on the prevention of harm, such as transmission of infectious disease transmission and overdose death, with attention and focus on connecting individuals to treatment, peer support and other recovery services. Harm reduction programs are an effective way to build connections with individuals who may benefit from treatment that can help facilitate initiation to services over time. For example, syringe service programs and other evidence-informed programs can reduce harms associated with intravenous drug use.
Additionally, the South Carolina Center of Excellence in Addiction provides technical assistance and training and education to South Carolina’s practitioners and community leaders.