Diagnosing Opioid Use Disorder
Background
Despite the opioid-related overdose and mortality crisis in South Carolina and throughout the country, opioid use disorder remains under diagnosed. Estimates suggest that as many as one-third of Americans with opioid use disorder have never been diagnosed with the condition. Without a diagnosis, the health care system misses important opportunities to offer treatment and other resources people need to achieve recovery from addiction.
Select map to display
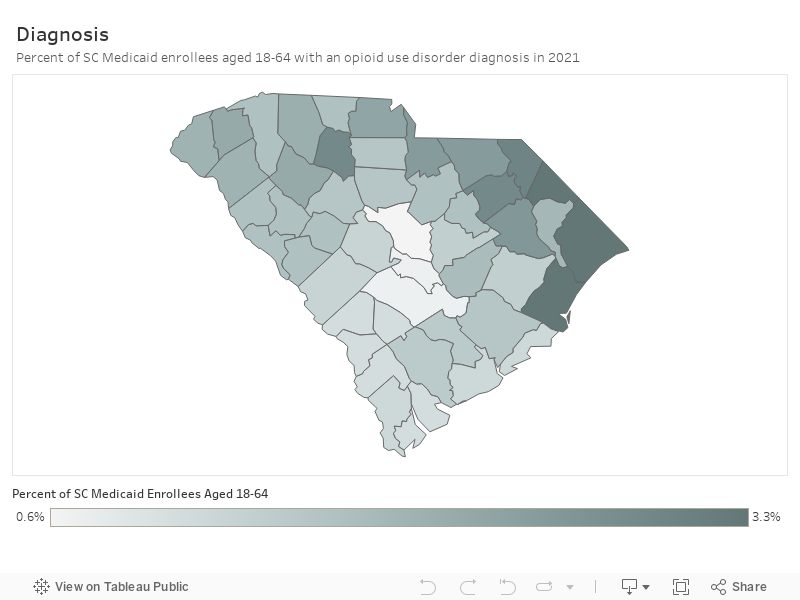
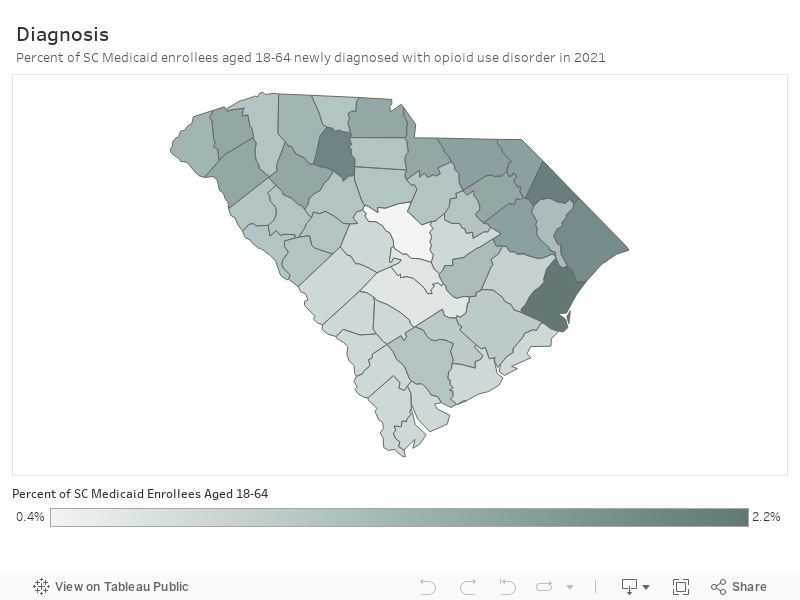
Percent of SC Medicaid enrollees aged 18-64 with an OUD:
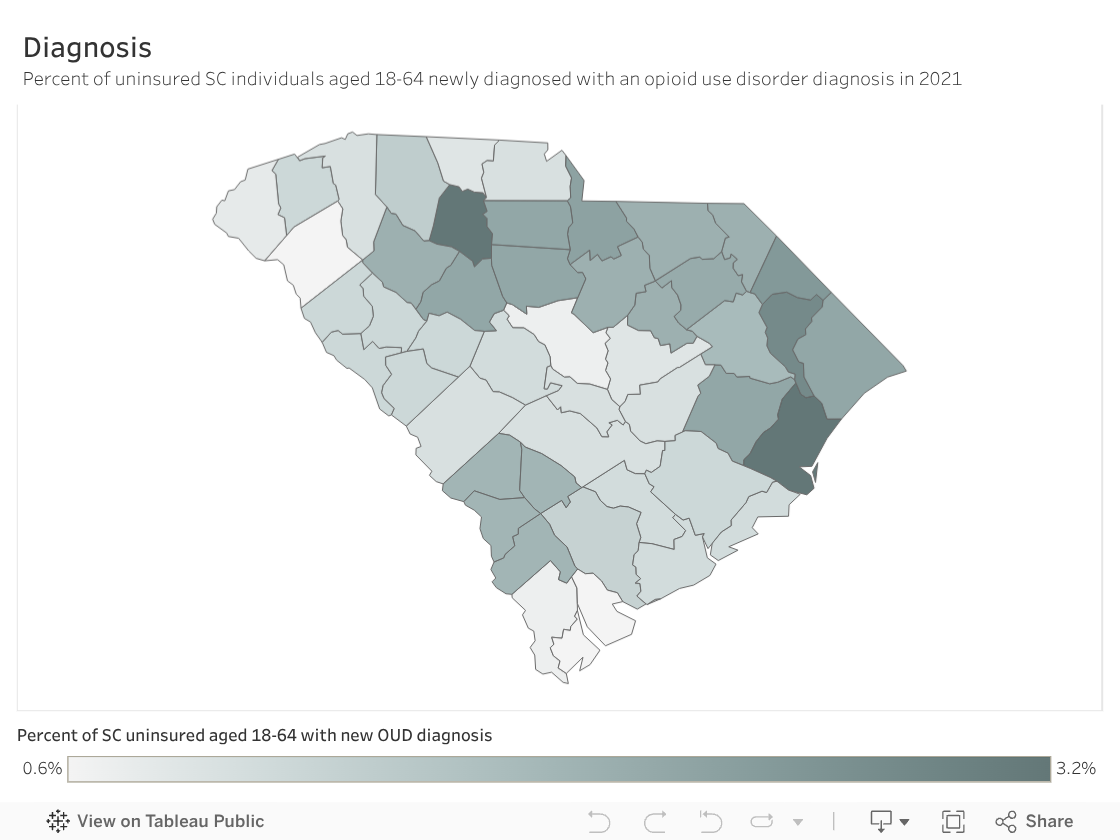
Percent of uninsured SC individuals aged 18-64
Background
Despite the opioid-related overdose and mortality crisis in South Carolina and throughout the country, opioid use disorder remains under diagnosed. Estimates suggest that as many as one-third of Americans with opioid use disorder have never been diagnosed with the condition.[i],[ii] Without a diagnosis, the health care system misses important opportunities to offer treatment and other resources people need to achieve recovery from addiction.How This Dashboard Measures Diagnosing Opioid Use Disorder
For this analysis, we included adults who were diagnosed with opioid use disorder during 2021. This includes people who have received multiple diagnoses, potentially starting before 2021, as well as people who received a new diagnosis in that year. We define a new diagnosis as an opioid use disorder diagnosis with a clean 2-month lookback window – that is, there were no opioid use disorder diagnoses or treatments in the prior two months for that patient. This doesn’t necessarily mean that the patient never had been diagnosed before, only that they were treatment naive for the preceding two months. This new diagnosis represents an opportunity for the medical system to engage this patient in treatment for their disorder, which usually happens immediately after diagnosis if it happens at all. We compiled a list of relevant diagnosis codes from the Centers for Medicare and Medicaid Services Chronic Conditions Warehouse and augmented this with other relevant diagnosis codes. We removed all codes that represented opioid poisoning or adverse events, as we wanted to focus specifically on opioid use disorder.Story Behind the Data
In 2021, an estimated 2.5 million people aged 18 years or older in the United States had opioid use disorder. It is estimated that nationwide, roughly 5% of adult Medicaid enrollees have an opioid use disorder. This equates to over one million Medicaid enrollees. However, among adults at least 18 years old, only 3.7%[iii] have a diagnosis of opioid use disorder. Among Medicaid enrollees, rates of diagnosis are even lower—approximately 3.0%.[iv] Our data show that South Carolina falls far below the national average in rates of diagnosis for opioid use disorder. Nationally, 4% of Americans have opioid use disorder.[v] Of adults aged 18-64 enrolled in South Carolina Medicaid, an average of 1.79% have an opioid use disorder diagnosis. Of uninsured adults seen by healthcare providers in a County Alcohol and Drug Authority or Opioid Treatment Program or the emergency department, 1.29% had a new opioid use disorder diagnosis in 2021. In summary, more than half of South Carolinians living with an active, untreated opioid use disorder are going undiagnosed. These data also show that opioid use disorder diagnosis rates vary substantially across counties in the state, ranging from a low of just 0.01% to a high of 3.34%. Overall, diagnosis rates are lowest in the state’s Midlands and Low Country regions, and highest in the Pee Dee region. It is important to note that differences in diagnosis rates likely reflect not only differences in health care system practices, but also variation in the underlying prevalence of opioid use disorder in different areas of the state. Thus, while understanding differences in diagnosis rates is important to improving the Cascade of Care, these measures should not be used as a metric by which to evaluate overall healthcare system performance.What Works
Identifying and diagnosing opioid use disorder represents an opportunity for clinicians to initiate potentially life-saving interventions. Primary care centers, hospital emergency departments, trauma centers, and other community settings provide opportunities for diagnosis and early intervention.-
- Implement screenings in health care settings and use evidence-based standardized approaches to identify opioid use disorder. Training clinicians in how to identify opioid use disorder is key. Using an evidence-based, standardized approach to identifying opioid use disorder can help optimize care and reduce stigma. Screening, Brief Intervention, and Referral to Treatment (SBIRT) is an evidence-based approach for intervening at all stages of substance use disorder, from identifying the needs of the patient to connecting them to treatment. A variety of screening tools[vi],[vii],[viii],[ix] can be used to identify opioid use disorder across health care settings.
- Implement evidence-based early intervention programs in schools. Evidence-based school or youth programs can prevent drug misuse. Schools can use this Evidence-Based Program Guidance for Substance Use Prevention Education in Schools to identify programs and strategies that have demonstrated effectiveness. The South Carolina Guide to Approved Uses for Investing Opioid Settlement Funds also identifies a number of evidence-based school programs that are shown to be effective in identifying children and adolescents in need of early intervention and treatment.
- Encourage interventions by first responders to connect at-risk individuals to behavioral health services and support (e.g. prearrest diversion programs, post-overdose response teams). First responders routinely interface with people with opioid use disorder and play a critical role in assisting individuals who have overdosed or experienced other adverse consequences of opioid use. Training first responders to participate in pre-arrest diversion programs, post-overdose response teams, or similar strategies that connect at-risk individuals to behavioral health services and supports can help connect those with opioid use disorder to treatment. For example, South Carolina’s Community Outreach Paramedic Education Programuses referrals from first responders or hospitals to identify overdose survivors for follow up visits by a multidisciplinary team that provides educational materials and “warm handoffs” to drug treatment and peer support.
References
[i] NIDA. Only 1 in 5 U.S. adults with opioid use disorder received medications to treat it in 2021. National Institute on Drug Abuse website. https://nida.nih.gov/news-events/news-releases/2023/08/only-1-in-5-us-adults-with-opioid-use-disorder-received-medications-to-treat-it-in-2021. August 7, 2023 Accessed August 2, 2024.
[ii] Keyes KM, Rutherford C, Hamilton A, et al. What is the prevalence of and trend in opioid use disorder in the United States from 2010 to 2019? Using multiplier approaches to estimate prevalence for an unknown population size. Drug Alcohol Depend Rep. 2022;3:100052. doi:10.1016/j.dadr.2022.100052
[iii] https://jamanetwork.com/journals/jama/fullarticle/2820545?guestaccesskey=184f080c-dabe-4323-8b90-b037b7229b6f
[iv] https://jamanetwork.com/journals/jama-health-forum/fullarticle/2806516
[v] https://www.cdc.gov/mmwr/volumes/73/wr/mm7325a1.htm
[vi] Ducharme J, Moore S. Opioid Use Disorder Assessment Tools and Drug Screening. Mo Med. 2019;116(4):318-324.
[vii] https://injurycenter.umich.edu/opioid-overdose/michigan-safer-opioid-prescribing-toolkit/post-overdose-toolkit/screening-for-oud/
[viii] https://nida.nih.gov/nidamed-medical-health-professionals/screening-tools-resources/chart-screening-tools
[ix] https://www.cdc.gov/overdose-prevention/media/pdfs/pubs/Linkage-to-Care-Resource-for-Action-508.pdf