Beginning Medication Treatment
Background
As soon as a patient is identified with opioid use disorder, it should be addressed to ensure efficient access to evidence-based treatment and support services. Left untreated, opioid use disorder can result in a decline in mental health and physical health, adverse social and economic consequences, and elevated risk of overdose and drug-related mortality.
Select map to display
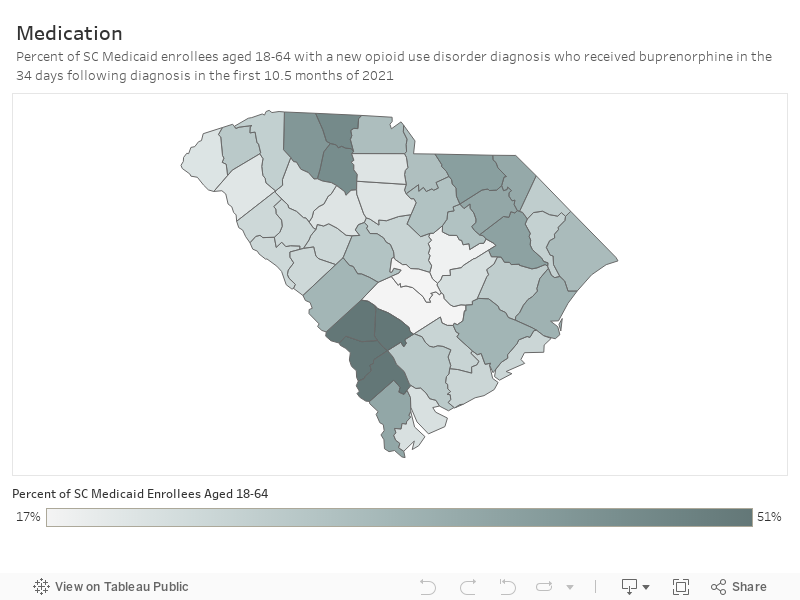
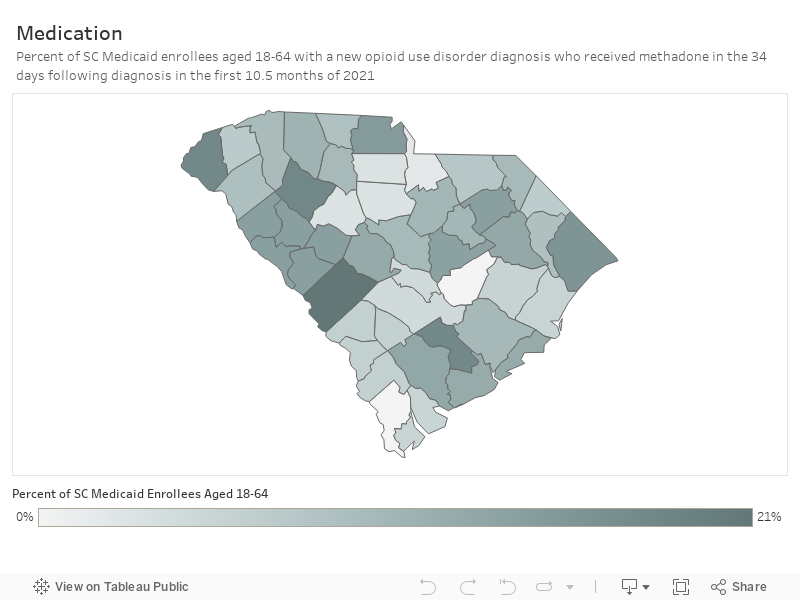
Percent of SC Medicaid enrollees aged 18-64 with a new OUD diagnosis
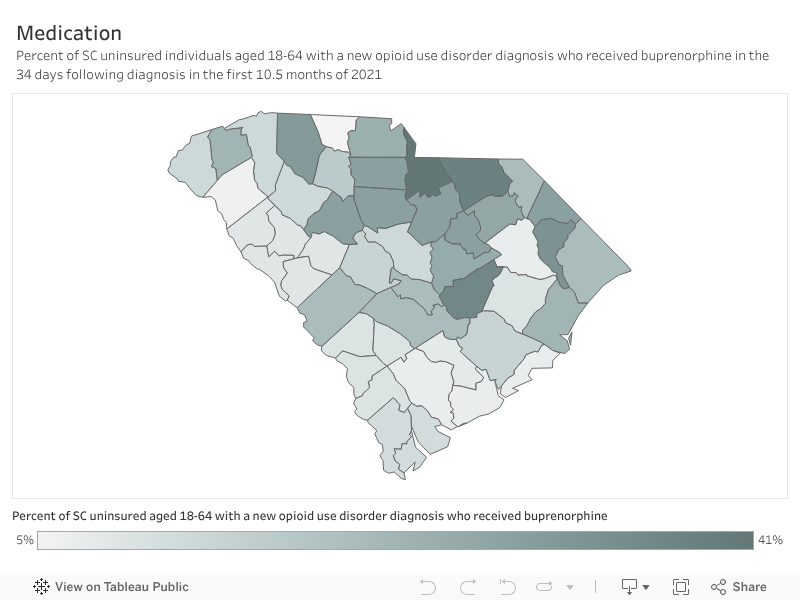
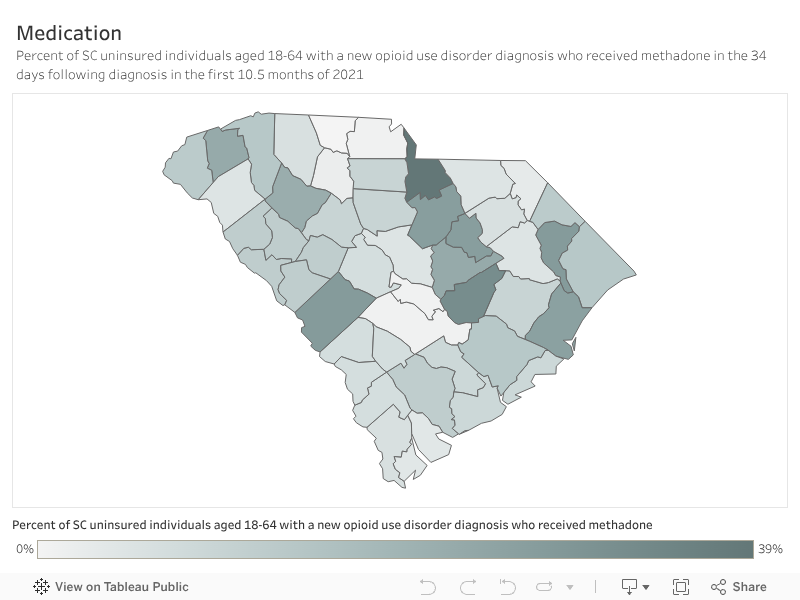
Percent of uninsured SC individuals aged 18-64 with a new OUD diagnosis
Background
As soon as a patient is identified with opioid use disorder, it should be addressed to ensure efficient access to evidence-based treatment and support services. Left untreated, opioid use disorder can result in a decline in mental and physical health, adverse social and economic consequences, and elevated risk of overdose and drug-related mortality. Medications for treatment of opioid use disorder are effective in facilitating recovery from addiction and are associated with reductions in overdose and opioid-related mortality.[i] Medications for treatment of opioid use disorder are used to reduce the intensity of withdrawal symptoms, curb cravings, and lessen the likelihood of use or relapse. The primary goal of medication is to assist the patient in reducing or eliminating use and achieving long-term recovery. Treating opioid use disorder with medication is evidence-based; those with opioid use disorder should begin medication immediately with or without concurrent psychosocial treatment. Medications for treating opioid use disorder are shown to:- Improve rates of patient survival
- Increase retention in treatment programs
- Decrease illicit opiate use and substance-related criminal involvement
- Increase patients’ ability to gain and maintain employment
- Improve outcomes in pregnancies affected by substance use
- Buprenorphine is classified as a “partial opioid agonist,” meaning it activates the brain’s opioid receptors but less intensely than full agonists like methadone. It provides relief up to a certain level, beyond which its effects do not increase, helping to prevent addictive euphoria and minimizing the risks of misuse, severe side effects, and overdose. Usually administered daily as a tablet or dissolvable film under the tongue, buprenorphine maintains its therapeutic effects while reducing potential dangers.
- Methadone is a medication classified as an “opioid agonist,” which activates brain receptors and alters the brain’s response to pain. It is available exclusively through federally-certified opioid treatment programs, and its use is highly regulated, often requiring daily administration. When taken as prescribed, methadone can alleviate opioid cravings, reduce withdrawal symptoms, support abstinence from other substances, and improve daily functioning.
- Naltrexone is a non-addictive medication that functions as an “opioid antagonist,” blocking the euphoric effects typically associated with opioid use. Commonly administered as a monthly extended-release injection under the brand name Vivitrol®, naltrexone has been proven to reduce opioid cravings, lower the risk of relapse and overdose, and support continued participation in addiction treatment programs.
How this Dashboard Measures Medication Receipt for Opioid Use Disorder
Only people with a new opioid use disorder diagnosis (i.e. no opioid use disorder diagnosis or treatment for the preceding 2 months) are included in these measures. These measures are adapted from National Committee for Quality Assurance’s (NCQA) Healthcare Effectiveness Data and Information Set (HEDIS) measures, which are widely used insurance plan performance measures. HEDIS measures are validated, claims-based measures that give a standardized format to compare health system and plan performance across states and years. The NCQA and National Quality Forum (NQF) provide guidelines for creation of these variables that help standardize measures across plans, states, and research teams. Cutoffs and windows for inclusion – such as 14 days, 34 days, and 10.5 months – are based on clinical consensus from NCQA research and HEDIS measure development. We did not include NDC or treatment codes for methadone or buprenorphine formulations used primarily for pain management. We did examine injectable naltrexone usage but did not include it in this analysis due to very low prevalence. The best opportunity to engage a patient in treatment is immediately following initial diagnosis. Early engagement with treatment, including medication, decreases risk of overdose and death. Medication is an important tool to treat opioid use disorder, and those who take medications have fewer cravings and are more likely to stay in treatment.Story Behind the Data
Fewer than half (42%) of adults with a new opioid use disorder enrolled in Medicaid, and fewer than a quarter (22%) of uninsured adults, received any medication for treatment.
Among South Carolina adults enrolled in Medicaid or uninsured who are aged 18–64 with a new opioid use disorder diagnosis in 2021:
- Medicaid adult enrollees: 31.0% received buprenorphine and 11.5% received methadone.
- Uninsured adults (who received care in County Alcohol and Drug Authority or Opioid Treatment Program or the emergency department): 19.0% received buprenorphine and 12.3% received methadone.

In summary, of South Carolina Medicaid enrollees aged 18-64 with a new opioid use disorder diagnosis in 2021, two in five people received medication for treatment within a timely manner. Of uninsured adults who received a new opioid use disorder diagnosis at a County Alcohol and Drug Authority or Opioid Treatment Program or an emergency department in 2021, one in five people received medication for treatment in a timely manner.
In other words, 60% of Medicaid enrollees and 80% of uninsured with opioid use disorder are not receiving timely medication for treatment.
Use of medication for opioid use disorder rates vary substantially across counties in the state. Overall, medication treatment rates are lowest in the Low Country region and highest in the Pee Dee and Midlands regions. Additionally, buprenorphine was distributed far more frequently than methadone. Injectable naltrexone is used very infrequently in South Carolina, and throughout the United States, and therefore is not included in the data reported on this dashboard.
What Works
Despite the strong evidence for the effectiveness of opioid use disorder treatment, there are numerous barriers that prevent individuals from engaging in treatment. A multi-pronged approach is needed to increase access and engagement of evidence-based treatment for opioid use disorder. Strategies include:- Expand treatment capacity by increasing the number of health care providers willing to prescribe buprenorphine. All practitioners with a current Drug Enforcement Administration registration that includes Schedule III authority can prescribe buprenorphine, with the 2023 removal of the federally required Drug Addiction Treatment Act of 2000 waiver (X-waiver) that may have previously limited prescribing. Given the high burden, morbidity, and mortality of opioid use disorder, it is important that all clinicians become familiar with the medications to treat opioid use disorder and that these medications become a routine part of medical practice.[ii] Clinicians can also utilize the South Carolina Center of Excellence in Addiction clinician ‘warmline’ for free, confidential, clinician-to-clinician consultation on medication management 9am – 5pm ET (Mon – Fri): 864-914-1301. The American Society of Addiction Medicine criteria is the most widely used and comprehensive set of standards for placement, continued service, and transfer of patients with addiction and co-occurring conditions. They also developed this National Practice Guideline for the Treatment of Opioid Use Disorder to provide information on evidence based treatment of opioid use disorder.
- Build and strengthen collaborative referral relationships between opioid treatment programs and other treatment providers. Strengthening collaborative referral relationships between opioid treatment programs and other treatment providers is essential for delivering holistic care to individuals with opioid use disorder. These partnerships ensure seamless transitions between various treatment modalities, improving continuity of care and enhancing patient outcomes. Effective collaboration also helps address a wide range of needs, from mental health to social services, by integrating multiple perspectives and resources. Moreover, robust referral networks can identify and bridge gaps in treatment, leading to more comprehensive and effective support for patients throughout their recovery journey.