
Retention in Treatment
Background
Research suggests that the longer a patient is engaged in treatment the better their long-term prognosis will be, and longer treatment engagement is associated with more positive outcomes. Yet retaining patients in care is a challenge for many health care systems, and improving retention has been identified as an important quality indicator for substance use disorder treatment programs.
Select map to display
Percent of SC Medicaid enrollees aged 18-64 who initiated:
Uninsured SC individuals aged 18-64 who initiated:

Background
Research suggests that the longer a patient is engaged in treatment the better their long-term prognosis will be, and longer treatment engagement is associated with more positive outcomes.[i] Yet retaining patients in care is a challenge for many health care systems, and improving retention has been identified as an important quality indicator for substance use disorder treatment programs.[ii]
How this Dashboard Measures Retention in Treatment for Opioid Use Disorder
Only people who initiated treatment after an opioid use disorder diagnosis are included in these measures. These measures adapted from National Committee for Quality Assurance’s (NCQA) Healthcare Effectiveness Data and Information Set (HEDIS) measures, which are widely used insurance plan performance measures. HEDIS measures are validated, claims-based measures that give a standardized format to compare health system and plan performance across states and years. The NCQA and National Quality Forum (NQF) provide guidelines for creation of these variables that help standardize measures across plans, states, and research teams. Cutoffs and windows for inclusion – such as 14 days, 34 days, and 10.5 months – are based on clinical consensus from NCQA research and HEDIS measure development. We require consistent treatment with medication and/or psychosocial therapy without a gap of longer than 7 days for a 90-day period to count towards retention in treatment. This 90-day period does not necessarily need to immediately follow diagnosis and initiation. A patient may hypothetically be diagnosed and initiate treatment, have a lapse in treatment, and shortly after restart and be retained in treatment. Retention in psychosocial and pharmacological treatment helps patients manage their illness over the long term and work towards remission.
Story Behind the Data
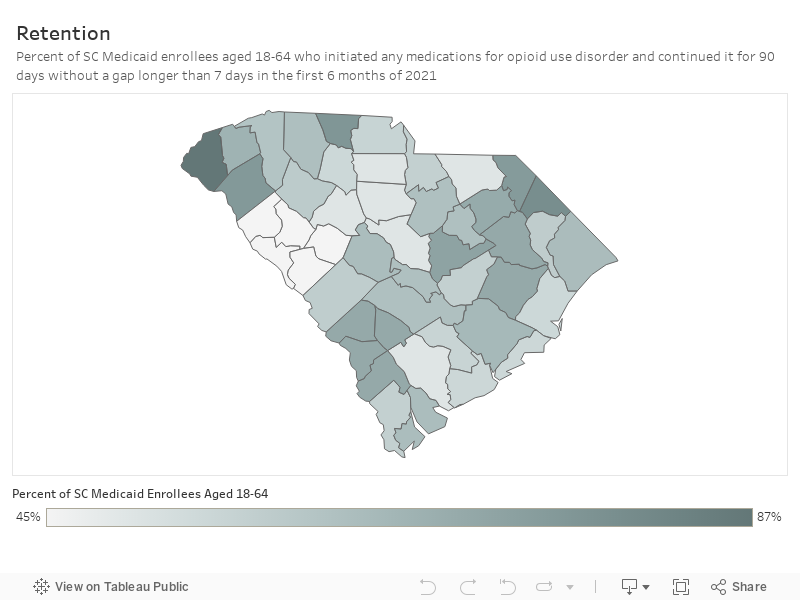
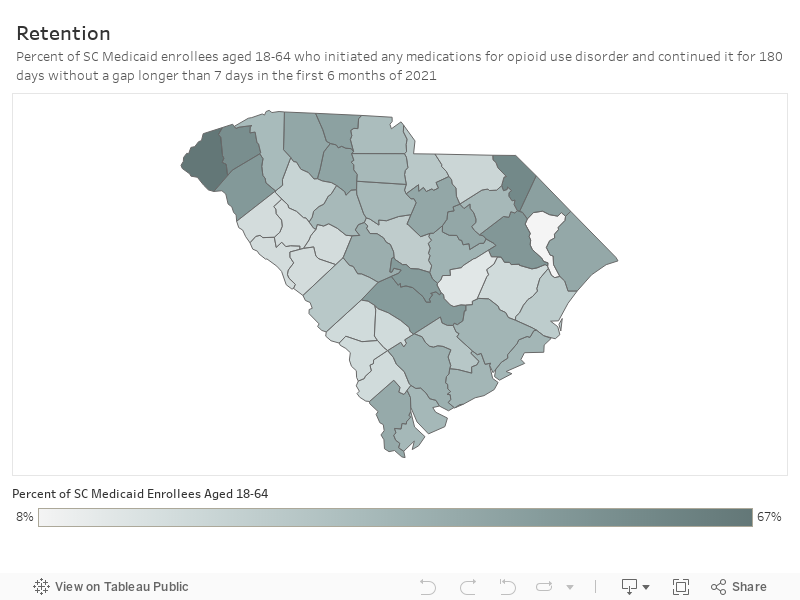
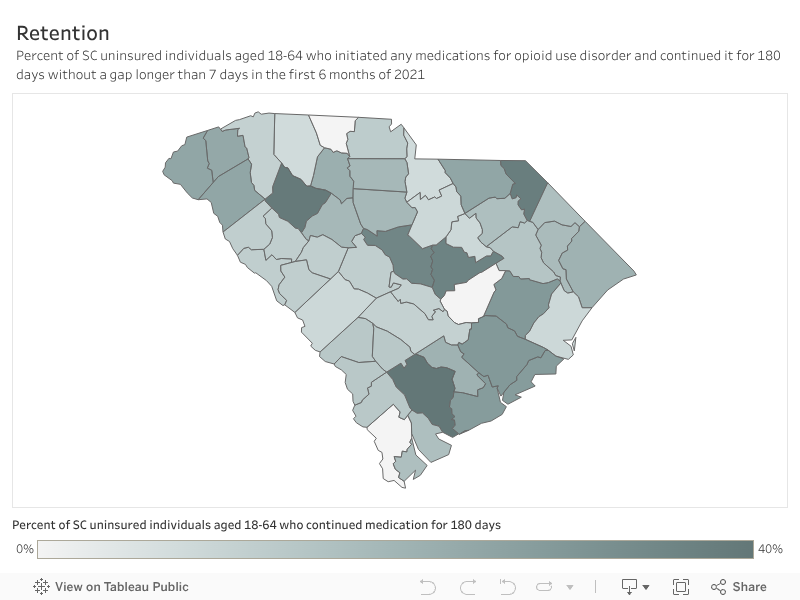
Over half (63%) of adults with a new opioid use disorder enrolled in Medicaid, and fewer than half (41%) of uninsured adults, were retained in any medication treatment. One third (33%) of adults with a new opioid use disorder enrolled in Medicaid, and about one quarter (24%) of uninsured adults, were retained in any medication treatment.
Among South Carolina adults enrolled in Medicaid or uninsured who are aged 18–64 with a new opioid use disorder diagnosis in 2021:
- Medicaid adult enrollees:
- 62.6% remained on medication treatment for 90 days without a gap longer than 7 days
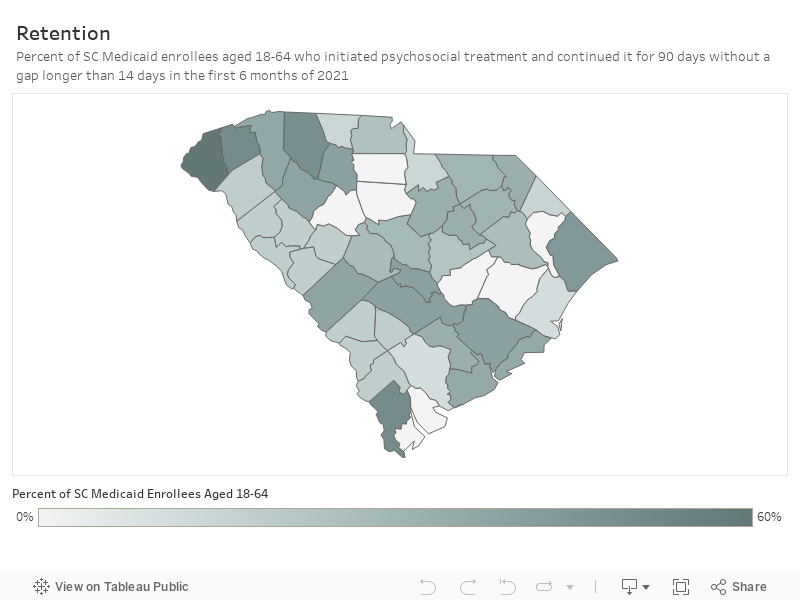
- 32.5% continued psychosocial treatment for 90 days without a gap longer than 14 days
- Uninsured adults (who received care in County Alcohol and Drug Authority or Opioid Treatment Program or the emergency department):
- 40.6% remained on medication treatment for 90 days without a gap longer than 7 days
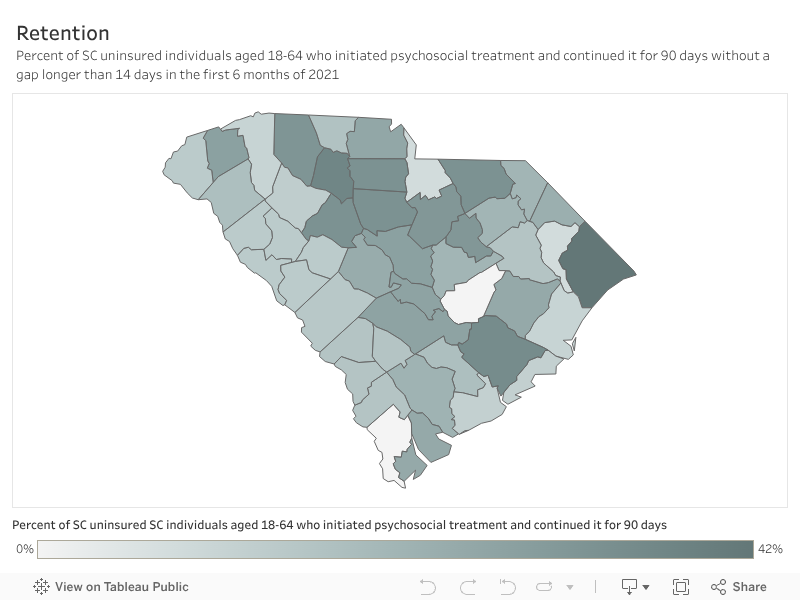
- 23.6% continued psychosocial treatment for 90 days without a gap longer than 14 days
In summary, of South Carolina Medicaid enrollees aged 18-64 with a new opioid use disorder diagnosis in 2021, three in five people were adequately retained in medication treatment. Of uninsured adults who received a new opioid use disorder diagnosis at a County Alcohol and Drug Authority or Opioid Treatment Program or an emergency department in 2021, two in five people were adequately retained in medication treatment.


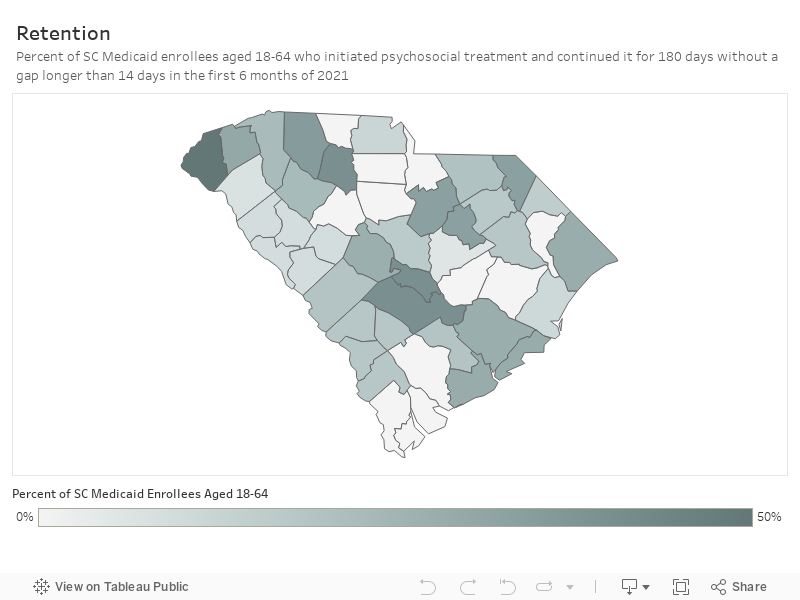
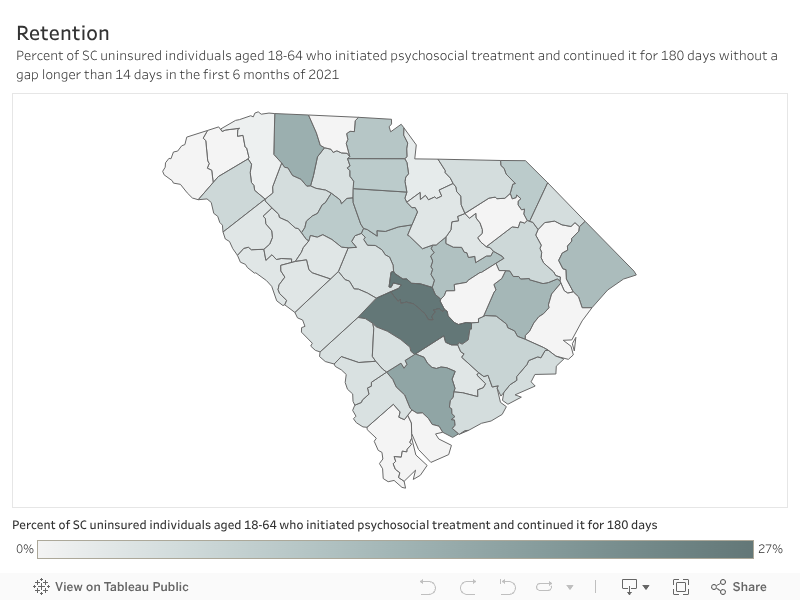
Of South Carolina Medicaid enrollees aged 18-64 with a new opioid use disorder diagnosis in 2021, fewer than one in three people were adequately retained in psychosocial treatment. Of uninsured adults who received a new opioid use disorder diagnosis at a County Alcohol and Drug Authority or Opioid Treatment Program or an emergency department in 2021, fewer than one in four were adequately retained in psychosocial treatment.
In other words, 37% of Medicaid enrollees and 60% of uninsured with opioid use disorder are not adequately retained in medication treatment. Additionally, 67% of Medicaid enrollees and 76% of uninsured with opioid use disorder are not adequately retained in psychosocial treatment.
Treatment retention rates vary widely across South Carolina counties for Medicaid enrollees or uninsured individuals newly diagnosed with opioid use disorder in 2021. The percentage of individuals who remained on medication treatment for 90 days without a gap over 7 days ranged narrowly from 85.7% to 86.7%. Psychosocial treatment retention showed greater variation, ranging from 0% to 64.3%.
Regionally, the Midlands had the lowest medication retention rates. We know longer retention on medication for opioid use disorder reduces morbidity and mortality, but improving retention remains a difficult for the state.
What Works
Research on what improves retention in opioid use disorder treatment is lacking. Despite limited evidence, some approaches have promising results[iii]:
- Provide services to address barriers to remaining in treatment, such as transportation and childcare. Barriers such as lack of transportation or childcare can make it challenging to access necessary services for engaging in opioid use disorder treatment. When logistical challenges are addressed, patients are more likely to attend appointments and adhere to treatment plans, leading to better outcomes. Additionally, reducing these barriers fosters a more supportive environment, encouraging patients to seek and remain in treatment consistently. Increasing telehealth options and mobile methadone programs can reduce common barriers to care and reach people in need across larger distances.
- Ensure care is patient centered and continue shared decision-making practices with patients around treatment initiation and retention. Patient-centered care is an approach to healthcare that prioritizes the needs, preferences, and values of the patient in all aspects of their care. This approach fosters a stronger therapeutic alliance, enhancing patient engagement and adherence to treatment plans. By involving patients in decisions about their care, they are more likely to remain committed to their treatment and feel empowered in their recovery journey. Additionally, shared decision-making helps tailor interventions to each individual’s circumstances, improving overall treatment outcomes and satisfaction.
- Implement treatment programs that include the use of health IT (e.g. tele-health, online programs). Opioid use disorder treatment programs that include the use of health IT may be equally as effective as those delivered using traditional, exclusively in-person approaches and can reduce barriers in access to care. Health IT tools can also support personalized care through data-driven insights, helping to tailor interventions to individual needs and preferences. Additionally, remote monitoring and digital reminders can help patients adhere to their treatment plans and manage their recovery more effectively.
Additionally, the South Carolina Center of Excellence in Addiction provides technical assistance and training and education to South Carolina’s practitioners and community leaders.
References
[i] https://www.nih.gov/news-events/news-releases/methadone-buprenorphine-reduce-risk-death-after-opioid-overdose
[ii] Jhanjee S. (2014). Evidence based psychosocial interventions in substance use. Indian journal of psychological medicine, 36(2), 112–118. https://doi.org/10.4103/0253-7176.130960
[iii] https://effectivehealthcare.ahrq.gov/sites/default/files/pdf/mat-retention-strategies-rapid-review-1.pdf